
Shoulder Pain Physical Therapy in Roswell, GA: The Most Overlooked Cause — And How We Actually Fix It
- Dr. William Duncan PT, DPT

- 5 days ago
- 7 min read

You've iced it. You've rested it. Maybe you've even done a few shoulder exercises you found on YouTube. And yet the shoulder pain is still there — grinding, aching, or shooting every time you reach overhead, throw, press, or just try to sleep on your side. Here's what most people don't hear from their doctor, their chiropractor, or the big-box PT clinic: the shoulder itself often isn't the real problem. At Southeast Physical Therapy — the destination for shoulder pain physical therapy in Roswell, GA that goes beyond the standard protocol — we see this pattern constantly.
Patients come in frustrated; some having dealt with the same shoulder for months. A few have had cortisone injections. Nearly all have been told to rest and take anti-inflammatories. When we do a thorough evaluation, the answer is often coming from somewhere the previous provider never assessed.
The Most Overlooked Cause of Shoulder Pain: Myofascial Trigger Points
Myofascial trigger points are tight, hypersensitive knots within a muscle that don't just hurt locally — they refer pain to predictable, distant locations. That's the part that gets missed. A trigger point in your neck can produce what feels exactly like a rotator cuff problem. A trigger point in your lat or triceps can create deep aching pain at the back of the shoulder that mimics bursitis. A trigger point in your biceps tendon region can drive anterior shoulder pain that looks like impingement on every clinical test.
The result: the shoulder gets all the treatment attention while the actual source of pain sits untouched in a muscle nobody examined.
This doesn't show up on MRI. It doesn't show up on X-ray. It requires a clinician with their hands on the tissue, understanding referral patterns, and taking the time to trace the pain backward to its origin.
Where the Pain Is Actually Coming From
Cervical Spine and Upper Trapezius
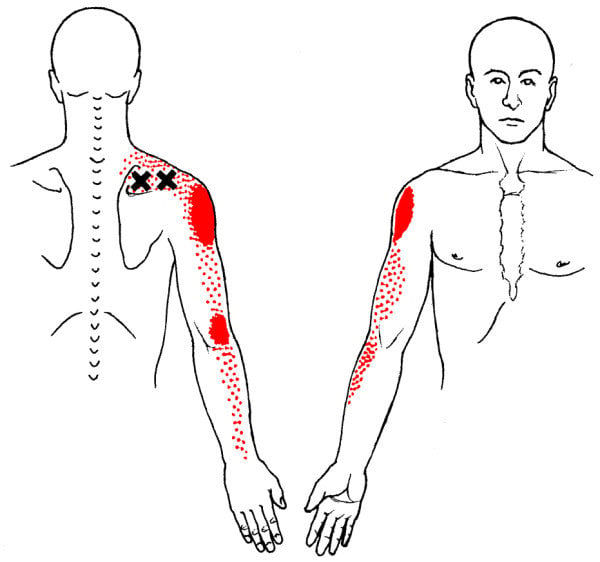
The cervical spine is one of the most common sources of referred shoulder pain — and one of the most commonly missed. Trigger points in the upper trapezius characteristically refer pain up into the neck and out toward the top of the shoulder. The levator scapulae refers pain to the angle of the neck and the medial border of the shoulder blade, producing that deep ache people describe as "knots" that never seem to release. The scalenes — a group most clinicians skip entirely — can refer pain down the outer arm and into the shoulder in a pattern that closely mimics cervical radiculopathy (nerve pain) or rotator cuff pathology.
If a patient has shoulder pain and nobody has assessed the cervical spine and the muscles that attach to it, the evaluation is incomplete.
Rotator Cuff Muscles
The rotator cuff itself is a common trigger point location, but the referral patterns matter more than where the tenderness is found.

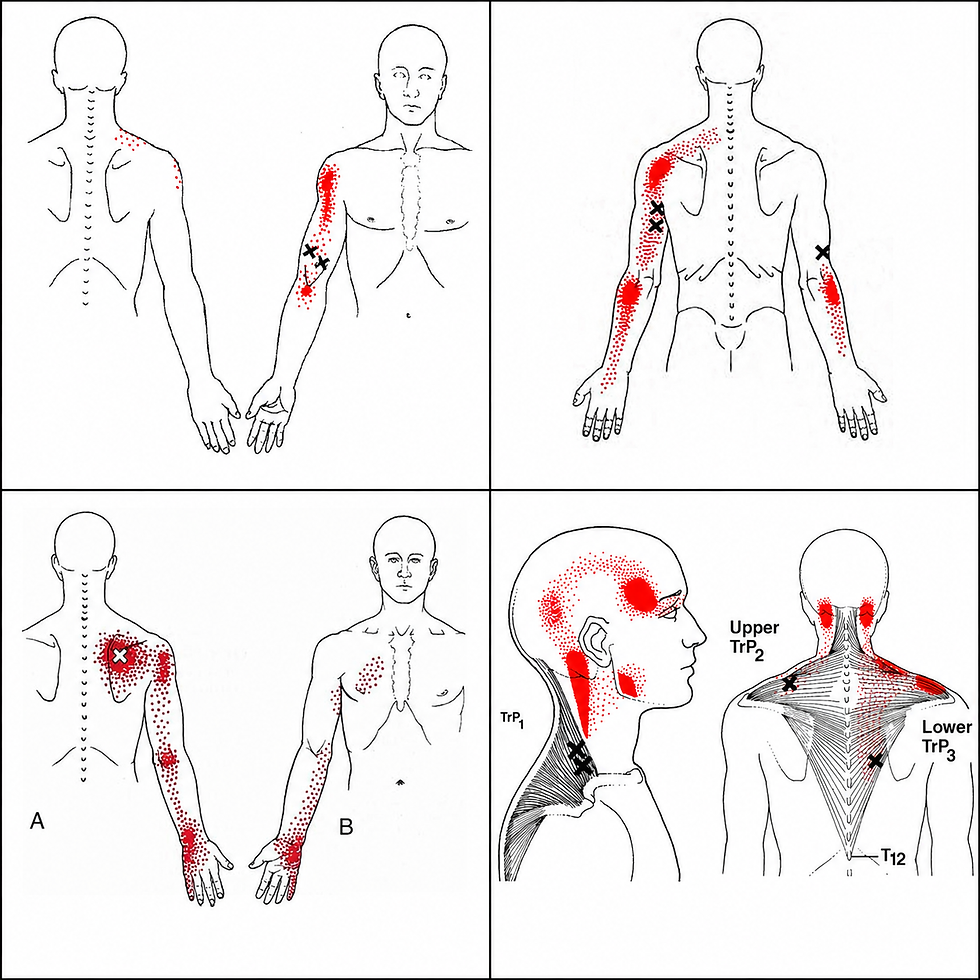
The infraspinatus is the most clinically significant: active trigger points here refer pain deep into the front of the shoulder and down the outer arm — a pattern so consistent that it's frequently mistaken for bicipital tendinopathy or subacromial impingement. Patients will point to the front of their shoulder, get treated there for months, and never improve because the infraspinatus was never addressed.
The supraspinatus refers pain to the mid-deltoid and lateral elbow.
Each of these has a distinct pattern, and treating shoulder pain without mapping them is guesswork.
Latissimus Dorsi
The lat is a massive muscle with a broad attachment footprint — and its trigger point referral pattern is almost always overlooked in shoulder evaluations.

Active trigger points in the latissimus dorsi refer pain to the inferior angle of the shoulder blade, the posterior shoulder, and down the inner arm into the fourth and fifth fingers. Patients with this pattern often describe a vague, diffuse aching at the back of the shoulder that worsens with reaching overhead or across the body. Because it doesn't fit neatly into a rotator cuff or labral diagnosis, it gets labeled as "nonspecific shoulder pain" — and treated accordingly, which is to say, not effectively.
Triceps
The triceps is another underappreciated contributor to posterior and lateral shoulder pain. Trigger points in the long head of the triceps refer pain to the posterior shoulder and the lateral elbow.

Patients who report shoulder pain that extends down the back of the arm, or who have both posterior shoulder complaints and lateral elbow sensitivity, often have active triceps trigger points driving the picture. This is particularly common in lifters and throwing athletes who load the triceps heavily in extension and overhead pressing patterns.
Biceps Brachii
The biceps contributes to anterior shoulder pain through two mechanisms. The long head tendon runs through the bicipital groove at the front of the shoulder and is a legitimate pain source — but trigger points in the biceps belly itself also refer pain to the anterior shoulder and the elbow pit.

In practice, the two get conflated constantly. A patient presents with anterior shoulder pain, gets diagnosed with bicipital tendonitis, does months of eccentric loading, and doesn't improve — because the muscle belly above was the actual generator, not the tendon.
Why This Gets Missed
Identifying myofascial trigger points and their referral patterns requires time, trained hands, and a systematic approach to the soft tissue that goes well beyond a standard orthopedic evaluation. Most clinical encounters don't include any of that. A 10-minute appointment built around range of motion testing and impingement special tests will almost never surface a trigger point in the infraspinatus or scalenes as the diagnosis — even when that's exactly what's driving the pain.
At our clinic, we treat one patient at a time — one-on-one with a Doctor of Physical Therapy for the entire session. That means we have the time to palpate systematically, follow referral patterns, assess the cervical spine and thoracic mobility in context, and build an accurate picture of what's actually generating the symptoms. That's a fundamentally different experience than what most patients get, and it's why patients who've been stuck for months frequently turn a corner quickly once the correct source is identified and treated.
How Shoulder Pain Physical Therapy in Roswell, GA Gets to the Root of It
If you're looking for shoulder pain physical therapy in Roswell, GA that actually identifies the source of the problem, here's what a thorough evaluation and treatment plan looks like at our clinic:
Systematic soft tissue assessment. We palpate the rotator cuff muscles, cervical musculature, lat, triceps, and biceps — not just the area that hurts. We're mapping the tissue, looking for active trigger points, and tracing referral patterns back to their source.
Dry needling and manual trigger point release. Once the active trigger points are identified, we address them directly. Dry needling is highly effective for deactivating trigger points that manual pressure alone can't fully resolve, particularly in deep muscles like the subscapularis and infraspinatus. For patients who prefer a non-needling approach, manual techniques achieve similar outcomes with consistent application.
Cervical spine assessment and treatment. If the neck is contributing — and it frequently is — we treat it. Joint mobilization, soft tissue work, and targeted exercise address cervical dysfunction that standard shoulder protocols miss entirely.
Progressive functional loading. Deactivating trigger points resolves the pain generator, but tissue capacity still needs to be restored. We rebuild strength and load tolerance progressively so the shoulder holds up under the demands of real life — training, work, sport, and sleep.
What This Looks Like in Practice
A fairly common presentation: a 38-year-old who lifts four days a week and has had right anterior shoulder pain for five months. Imaging showed mild supraspinatus tendinopathy. They've done two rounds of big-box PT focused on rotator cuff strengthening and posterior capsule stretching. No meaningful improvement.
On evaluation, we find active trigger points in the right infraspinatus with referral directly into the anterior shoulder — reproducing the exact pain they've been describing. Secondary active trigger points in the upper trapezius on the same refer into the lateral shoulder and arm. The supraspinatus tendinopathy on MRI is real, but it's been irritated by the altered mechanics created by the trigger points above it. Treating the tendon while the trigger points remain active is treating downstream of the problem.
After two sessions of dry needling to the infraspinatus and upper trap plus manual cervical work, the anterior shoulder pain is significantly reduced. From there, progressive loading restores the tissue capacity that months of pain and guarding had eroded.
That's not unusual. It's what happens when the actual pain source gets found.
Who This Applies To
Myofascial trigger points contribute to a wide range of shoulder presentations we treat regularly:
Anterior shoulder pain misdiagnosed as bicipital tendonitis
Posterior shoulder pain attributed to bursitis or labral pathology
Lateral shoulder and arm pain mimicking rotator cuff impingement
Shoulder pain with concurrent neck stiffness or upper trap tightness
Chronic shoulder pain that hasn't responded to standard PT
Post-surgical shoulder rehab where residual pain persists after structural healing
Overhead and throwing athlete shoulder pain
Gym-related shoulder injuries in pressing, pulling, and overhead patterns
If your shoulder pain has been diagnosed but hasn't resolved, the missing piece is likely in the soft tissue — and it's likely somewhere nobody has looked yet.
Southeast PT Serves All of North Atlanta
We're located in Roswell, GA and treat patients from across the North Atlanta area — including Alpharetta, Milton, East Cobb, Sandy Springs, Marietta, and Woodstock. Whether you found us searching for shoulder pain physical therapy in Roswell, GA or you were referred by someone who's trained here, you'll get the same thing: a DPT who takes the time to find what's actually wrong.
Our model is out-of-network. No divided attention, no aide-supervised exercise, no 40-minute wait for a 10-minute treatment. Every session is one-on-one with a DPT who knows your case and has a plan — because that's the only way this works.
Ready to Find Out What's Actually Going On?
If you've been managing shoulder pain and not getting the answers or results you need, a thorough evaluation is where it starts. We'll assess the tissue, trace the referral patterns, and build a plan to fix the actual problem — not manage the symptoms.
Book your evaluation at Southeast Physical Therapy in Roswell, GA



Comments